FAQs
Restorative Care
The pediatric dentist has an extra two to three years of specialized training after dental school, and is dedicated to the oral health of children from infancy through the teenage years. The very young, pre-teens, and teenagers all need different approaches in dealing with their behavior, guiding their dental growth and development, and helping them avoid future dental problems. The pediatric dentist is best qualified to meet these needs.
According to the American Academy of Pediatric Dentistry (AAPD), your child should visit the dentist by his/her 1st birthday. You can make the first visit to the dentist enjoyable and positive. Your child should be informed of the visit and told that the dentist and their staff will explain all procedures and answer any questions. The less to-do concerning the visit, the better.
It is best if you refrain from using words around your child that might cause unnecessary fear, such as needle, pull, drill or hurt. Pediatric dental offices make a practice of using words that convey the same message, but are pleasant and non-frightening to the child such as sleepy juice for the anesthetic, vacuum for the suction and so forth.
Tooth decay is the disease known as caries or cavities — a highly Preventable disease caused by many factors.
The answer is… everyone who has a mouth. We all host bacteria in our mouths which make everyone a potential target for cavities.
Risk factors that put a person at a higher risk for tooth decay include:
- Persons with diets high in sweets, carbohydrates, and sugars
- Persons who live in communities with limited or no fluoridated water supplies
- Children and senior citizens
It is very important to maintain the health of the primary teeth. Neglected cavities can and frequently do lead to problems which affect developing permanent teeth. Primary teeth, or baby teeth are important for
1). proper chewing and eating
2). providing space for the permanent teeth and guiding them into the correct position
3). and permitting normal development of the jaw bones and muscles
Primary teeth also affect the development of speech and add to an attractive appearance. While the front 4 teeth last until 6-7 years of age, the back teeth (cuspids and molars) aren’t replaced until age 10-13.
One serious form of decay among young children is baby bottle tooth decay. This condition is caused by frequent and long exposures of an infant’s teeth to liquids that contain sugar. Among these liquids are milk (including breast milk), formula, fruit juice and other sweetened drinks.
Putting a baby to bed for a nap or at night with a bottle other than water can cause serious and rapid tooth decay. Sweet liquid pools around the child’s teeth giving plaque bacteria an opportunity to produce acids that attack tooth enamel. If you must give the baby a bottle as a comforter at bedtime, it should contain only water. If your child won’t fall asleep without the bottle and its usual beverage, gradually dilute the bottle’s contents with water over a period of two to three weeks.
After each feeding, wipe the baby’s gums and teeth with a damp washcloth or gauze pad to remove plaque. The easiest way to do this is to sit down, place the child’s head in your lap or lay the child on a dressing table or the floor. Whatever position you use, be sure you can see into the child’s mouth easily.
The pulp of a tooth is the inner central core of the tooth. The pulp contains nerves, blood vessels, connective tissue and reparative cells. The purpose of pulp therapy in Pediatric Dentistry is to maintain the vitality of the affected tooth (so the tooth is not lost).
Dental caries (cavities) and traumatic injury are the main reasons for a tooth to require pulp therapy. Pulp therapy is often referred to as a “nerve treatment”, “children’s root canal”, “pulpectomy” or “pulpotomy”. The two common forms of pulp therapy in children’s teeth are the pulpotomy and pulpectomy.
A pulpotomy removes the diseased pulp tissue within the crown portion of the tooth. Next, an agent is placed to prevent bacterial growth and to calm the remaining nerve tissue. This is followed by a final restoration (usually a stainless steel crown).
A pulpectomy is required when the entire pulp is involved (into the root canal(s) of the tooth). During this treatment, the diseased pulp tissue is completely removed from both the crown and root. The canals are cleansed, disinfected and in the case of primary teeth, filled with a resorbable material. Then a final restoration is placed. A permanent tooth would be filled with a non-resorbing material.
Teething, the process of baby (primary) teeth coming through the gums into the mouth, is variable among individual babies. Some babies get their teeth early and some get them late. In general the first baby teeth are usually the lower front (anterior) teeth and usually begin erupting between the age of 6-8 months. See “Eruption of Your Child’s Teeth” for more details.
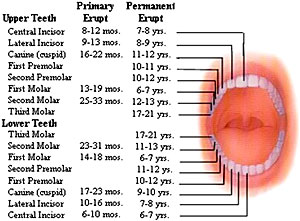
Eruption Of Your Child’s Teeth
Children’s teeth begin forming before birth. As early as 4 months, the first primary (or baby) teeth to erupt through the gums are the lower central incisors, followed closely by the upper central incisors. Although all 20 primary teeth usually appear by age 3, the pace and order of their eruption varies.
Permanent teeth begin appearing around age 6, starting with the first molars and lower central incisors. This process continues until approximately age 21.
Adults have 28 permanent teeth, or up to 32 including the third molars (or wisdom teeth).
Tooth Development
Preventive Care
Begin daily brushing as soon as the child’s first tooth erupts. A pea size amount of fluoride toothpaste can be used after the child is old enough not to swallow it. By age 4 or 5, children should be able to brush their own teeth twice a day with supervision until about age seven to make sure they are doing a thorough job. However, each child is different. Your dentist can help you determine whether the child has the skill level to brush properly.
Proper brushing removes plaque from the inner, outer and chewing surfaces. When teaching children to brush, place toothbrush at a 45 degree angle; start along gum line with a soft bristle brush in a gentle circular motion. Brush the outer surfaces of each tooth, upper and lower. Repeat the same method on the inside surfaces and chewing surfaces of all the teeth. Finish by brushing the tongue to help freshen breath and remove bacteria.
Flossing removes plaque between the teeth where a toothbrush can’t reach. Flossing should begin when any two teeth touch. You should floss the child’s teeth until he or she can do it alone. Use about 18 inches of floss, winding most of it around the middle fingers of both hands. Hold the floss lightly between the thumbs and forefingers. Use a gentle, back-and-forth motion to guide the floss between the teeth. Curve the floss into a C-shape and slide it into the space between the gum and tooth until you feel resistance. Gently scrape the floss against the side of the tooth. Repeat this procedure on each tooth. Don’t forget the backs of the last four teeth.
Good oral hygiene removes bacteria and the left over food particles that combine to create cavities. For infants, use a wet gauze or clean washcloth to wipe the plaque from teeth and gums. Avoid putting your child to bed with a bottle filled with anything other than water. See “Baby Bottle Tooth Decay” for more information.
For older children, brush their teeth at least twice a day. Also, watch the number of snacks containing sugar that you give your children.
The American Academy of Pediatric Dentistry recommends six month visits to the pediatric dentist beginning at your child’s first birthday. Routine visits will start your child on a lifetime of good dental health.
Your pediatric dentist may also recommend protective sealants or home fluoride treatments for your child. Sealants can be applied to your child’s molars to prevent decay on hard to clean surfaces.
Tooth brushing is one of the most important tasks for good oral health. Many toothpastes, and/or tooth polishes, however, can damage young smiles. They contain harsh abrasives which can wear away young tooth enamel. When looking for a toothpaste for your child make sure to pick one that is recommended by the American Dental Association. These toothpastes have undergone testing to insure they are safe to use.
Remember, children should spit out toothpaste after brushing to avoid getting too much fluoride. If too much fluoride is ingested, a condition known as fluorosis can occur. If your child is too young or unable to spit out toothpaste, consider providing them with a fluoride free toothpaste, using no toothpaste, or using only a “pea size” amount of toothpaste.
Fluoride is an element, which has been shown to be beneficial to teeth. However, too little or too much fluoride can be detrimental to the teeth. Little or no fluoride will not strengthen the teeth to help them resist cavities. Excessive fluoride ingestion by preschool-aged children can lead to dental fluorosis, which is a chalky white to even brown discoloration of the permanent teeth. Many children often get more fluoride than their parents realize. Being aware of a child’s potential sources of fluoride can help parents prevent the possibility of dental fluorosis.
Some of these sources are:
- Too much fluoridated toothpaste at an early age
- The inappropriate use of fluoride supplements
- Hidden sources of fluoride in the child’s diet
Two and three year olds may not be able to expectorate (spit out) fluoride-containing toothpaste when brushing. As a result, these youngsters may ingest an excessive amount of fluoride during tooth brushing. Toothpaste ingestion during this critical period of permanent tooth development is the greatest risk factor in the development of fluorosis.
Excessive and inappropriate intake of fluoride supplements may also contribute to fluorosis. Fluoride drops and tablets, as well as fluoride fortified vitamins should not be given to infants younger than six months of age. After that time, fluoride supplements should only be given to children after all of the sources of ingested fluoride have been accounted for and upon the recommendation of your pediatrician or pediatric dentist.
Certain foods contain high levels of fluoride, especially powdered concentrate infant formula, soy-based infant formula, infant dry cereals, creamed spinach, and infant chicken products. Please read the label or contact the manufacturer. Some beverages also contain high levels of fluoride, especially decaffeinated teas, white grape juices, and juice drinks manufactured in fluoridated cities. Another source of fluoride can be found in soft drinks at fast food restaurants, when blending the syrup and carbonation with the city water supply.
Parents can take the following steps to decrease the risk of fluorosis in their children’s teeth:
- Use baby tooth cleanser on the toothbrush of the very young child
- Place only a pea sized drop of children’s toothpaste on the brush when brushing
- Account for all of the sources of ingested fluoride before requesting fluoride supplements from your child’s physician or pediatric dentist
- Avoid giving any fluoride-containing supplements to infants until they are at least 6 months old ■ Obtain fluoride level test results for your drinking water before giving fluoride supplements to your child (check with local water utilities)
Topical fluoride is applied on cleaned tooth surfaces to strengthen teeth and help fight decay.
Children who benefit the most from fluoride are those at highest risk for dental decay. Risk Factors include a history of decay, high sucrose carbohydrate diet, orthodontic appliances and certain medical conditions such as dry mouth.
Parents are often concerned about the nocturnal(night time) grinding of teeth (bruxism). Often, the first indication is the noise created by the child grinding on their teeth during sleep. Or, the parent may notice wear (teeth getting shorter) to the dentition. One theory as to the cause involves a psychological component. Stress due to a new environment, divorce, changes at school; etc. can influence a child to grind their teeth. Another theory relates to pressure in the inner ear at night. If there are pressure changes (like in an airplane during take-off and landing when people are chewing gum, etc. to equalize pressure) the child will grind by moving his jaw to relieve this pressure.
The majority of cases of pediatric bruxism do not require any treatment. If excessive wear of the teeth (attrition) is present, then a mouth guard (night guard) may be indicated. The negatives to a mouth guard are the possibility of choking if the appliance becomes dislodged during sleep and it may interfere with growth of the jaws. The positive is obvious by preventing wear to the primary dentition.
The good news is most children outgrow bruxism. The grinding gets less between the ages 6-9 and children tend to stop grinding between ages 9-12. If you suspect bruxism, discuss this with your pediatrician or pediatric dentist.
Thumb sucking that persists beyond the eruption of the permanent teeth can cause problems with the proper growth of the mouth and tooth alignment. How intensely a child sucks on fingers or thumbs will determine whether or not dental problems may result. Children who rest their thumbs passively in their mouths are less likely to have difficulty than those who vigorously suck their thumbs.
- Instead of scolding children for thumb sucking, praise them when they are not
- Children often suck their thumbs when feeling insecure. Focus on correcting the cause of anxiety, instead of the thumb sucking
- Children who are sucking for comfort will feel less of a need when their parents provide comfort
- Reward children when they refrain from sucking during difficult periods, such as when being separated from their parents
- Your pediatric dentist can encourage children to stop sucking and explain what could happen if they continue
- If these approaches don’t work, remind the children of their habit by bandaging the thumb or putting a sock on the hand at night. Your pediatric dentist may recommend the use of a mouth appliance
You might not be surprised anymore to see people with pierced tongues, lips or cheeks, but you might be surprised to know just how dangerous these piercings can be.
There are many risks involved with oral piercings including chipped or cracked teeth, blood clots, or blood poisoning. Your mouth contains millions of bacteria, and infection is a common complication of oral piercing. Your tongue could swell large enough to close off your airway!
Common symptoms after piercing include pain, swelling, infection, an increased flow of saliva and injuries to gum tissue. Difficult-to-control bleeding or nerve damage can result if a blood vessel or nerve bundle is in the path of the needle.
So follow the advice of the American Dental Association and give your mouth a break – skip the mouth jewelry.
Tobacco in any form can jeopardize your child’s health and cause incurable damage. Teach your child about the dangers of tobacco.
Smokeless tobacco, also called spit, chew or snuff, is often used by teens who believe that it is a safe alternative to smoking cigarettes. This is an unfortunate misconception. Studies show that spit tobacco may be more addictive than smoking cigarettes and may be more difficult to quit. Teens who use it may be interested to know that one can of snuff per day delivers as much nicotine as 60 cigarettes. In as little as three to four months, smokeless tobacco use can cause periodontal disease and produce pre-cancerous lesions called leukoplakias.v If your child is a tobacco user you should watch for the following that could be early signs of oral cancer:
A sore that won’t heal
White or red leathery patches on the lips, and on or under the tongue
Pain, tenderness or numbness anywhere in the mouth or lips
Difficulty chewing, swallowing, speaking or moving the jaw or tongue; or a change in the way the teeth fit together
Because the early signs of oral cancer usually are not painful, people often ignore them. If it’s not caught in the early stages, oral cancer can require extensive, sometimes disfiguring, surgery. Even worse, it can kill. Help your child avoid tobacco in any form. By doing so, they will avoid bringing cancer-causing chemicals in direct contact with their tongue, gums and cheek
Developing malocclusions, or bad bites, can be recognized as early as 2-3 years of age. Often, early steps can be taken to reduce the need for major orthodontic treatment at a later age.
Stage I – Early Treatment: This period of treatment encompasses ages 2 to 6 years. At this young age, we are concerned with underdeveloped dental arches, the premature loss of primary teeth, and harmful habits such as finger or thumb sucking. Treatment initiated in this stage of development is often very successful and many times, though not always, can eliminate the need for future orthodontic/orthopedic treatment.
Stage II – Mixed Dentition: This period covers the ages of 6 to 12 years, with the eruption of the permanent incisor (front) teeth and 6 year molars. Treatment concerns deal with jaw malrelationships and dental realignment problems. This is an excellent stage to start treatment, when indicated, as your child’s hard and soft tissues are usually very responsive to orthodontic or orthopedic forces.
Stage III – Adolescent Dentition: This stage deals with the permanent teeth and the development of the final bite relationship.
When a child begins to participate in recreational activities and organized sports, injuries can occur. A properly fitted mouth guard, or mouth protector, is an important piece of athletic gear that can help protect your child’s smile, and should be used during any activity that could result in a blow to the face or mouth.
Mouth guards help prevent broken teeth, and injuries to the lips, tongue, face or jaw. A properly fitted mouth guard will stay in place while your child is wearing it, making it easy for them to talk and breathe.
Ask your pediatric dentist about custom and store-bought mouth protectors.
Early Orthodontic Care
Developing malocclusions, or bad bites, can be recognized as early as 2-3 years of age. Often, early steps can be taken to reduce the need for major orthodontic treatment at a later age.
Stage I – Early Treatment: This period of treatment encompasses ages 2 to 6 years. At this young age, we are concerned with underdeveloped dental arches, the premature loss of primary teeth, and harmful habits such as finger or thumb sucking. Treatment initiated in this stage of development is often very successful and many times, though not always, can eliminate the need for future orthodontic/orthopedic treatment.
Stage II – Mixed Dentition: This period covers the ages of 6 to 12 years, with the eruption of the permanent incisor (front) teeth and 6 year molars. Treatment concerns deal with jaw malrelationships and dental realignment problems. This is an excellent stage to start treatment, when indicated, as your child’s hard and soft tissues are usually very responsive to orthodontic or orthopedic forces.
Stage III – Adolescent Dentition: This stage deals with the permanent teeth and the development of the final bite relationship.
The alignments of teeth are often genetically determined. The child inherits the tooth size from one parent and the jaw size from the other parent. This may cause a discrepancy in the jaw and tooth size and lead to spacing or crowding of teeth. Orthodontic problems can also be caused by habits that apply forces on the developing dentition such as thumb sucking and finger sucking. Early loss of baby teeth can cause drifting of the adjacent teeth and prevent the permanent teeth to take the normal path of eruption and causing crowding and collapsed jaws.
Your pediatric dentist can help your child avoid oral habits that may create orthodontic problems.
Maintaining good oral hygiene is the key for successful orthodontic treatment. Brush your teeth carefully after every meal with fluoride toothpaste and a soft-bristled toothbrush, as food becomes easily lodged in the braces. Floss daily between the teeth and the braces. Maintain every 6 month cleanings by an oral health professional. Limit your sugar and starch intake, as debris left behind from these types of foods may turn into damaging acids, which, in addition to promoting plaque formation, may also be harmful to teeth and gums. Avoid hard and/or sticky snacks that may be difficult to remove from the orthodontic equipment in your mouth. This includes foods such as popcorn, hard or chew candy, caramel, and/or nuts.
Promptly contact with your pediatric dentist when an appliance breaks to keep orthodontic treatment on-time and on-track.
Emergency Care
To save the tooth, follow these steps:
- Rinse the tooth in tap water
- Avoid scrubbing the tooth
- Insert the tooth into the empty socket quickly
- If you are uncomfortable inserting the tooth, put the tooth in milk or water Get to the dentist immediately
Common dental emergencies
Chipped or Fractured teeth
Although teeth are the strongest substance in the whole body, they may chip or break due to various reasons. Some of the most common reasons are biting into something hard accidentally, tooth with a large filling, root canal treated tooth that is not capped and tooth undermined due to decay. What to expect?
Depending on the extent of fracture your tooth may be sensitive to temperature and pressure changes. Rinse your mouth gently with lukewarm water. Take a pain reliever if needed. See your dentist as soon as possible so he can determine the course of treatment.
How is it treated?
Fractures may involve only the superficial outer part of the tooth (enamel). In such a case your dentist may lightly polish the area to smooth the rough surfaces or place a filling and observe the tooth for further changes.
If the fracture involves the enamel and the inner sensitive dentin your dentist may have to place a crown due to the extent of involvement. This will protect the tooth and prevent further damage. Sometimes fractures may involve the enamel, dentin and the nerve tissue inside the tooth. This will necessitate a root canal treatment and a crown. If the crack extends beyond the gum line it may require a crown lengthening procedure, which involves removal of bone to grasp enough healthy structure for the crown.
However, if the crack extends to the root the tooth cannot be saved and will have to be removed.
Canker sores are shallow, painful sores in your mouth. They are usually red or may sometimes have a white coating over them. You may get them on the inside of your lips, the insides of your cheeks, the base of your gums or under your tongue. Canker sores are different from fever blisters, which usually are on the outside of your lips or the corners of your mouth.
Anyone can get canker sores, but women people in their teens and 20s get them more often. Canker sores may run in families, but they aren’t contagious. Causes of canker sores are unknown but they may be triggered by stress, poor nutrition, food allergies, spicy foods and menstrual periods.
Treatment
Canker sores usually go away without treatment. However, for pain relief your dentist may recommend medicines such as Anbesol, Oragel, Orabase and Zilactin-B, which may prevent your canker sores from becoming irritated by eating, drinking or brushing your teeth. These medicines can be applied directing on the sore with your finger tip or a Q-tip. Gently dry the sore with a swab before applying. Do not eat or drink anything for 30 minutes after applying.
Prevention
Unfortunately, causes of canker sore formation are unknown. However, using toothpaste that does not contain SLS (sodium lauryl sulphate), avoiding hard, crunchy or spicy foods and chewing gum may help reduce mouth irritation. Brushing your teeth after meals, using a soft toothbrush and flossing every day will also keep your mouth free of food that might cause a canker sore. If you get canker sores often, or if they’re very painful, talk to your dentist.
Operculitis
Operculitis is an inflammation of the gum tissue found over partially erupted teeth. The most frequent site is the mandibular third molar region. The heavy flap of gingival tissues covering portions of the tooth crown of the tooth makes an ideal pocket for debris accumulation and bacterial incubation. In the acute phase, pain and swelling in the area are prominent features. Symptoms of a sore throat and difficulty in swallowing may be present. A partial contraction of muscles of mastication, causing difficulty in opening the mouth (trismus), may also be experienced. Abscess formation in the area may occur, leading to marked systemic symptoms of general malaise and fever.
Treatment involves careful cleaning below the flap and saline irrigation. It may also require antibiotic therapy if the condition warrants. Your dentist may decide to incise the gingival flap to make the area self cleansable. If in the third molar area it may require the extraction of the tooth.